
What do the Origin of Life, a Hundred Billion Dollars, and a Viral Outbreak on a Cruise Ship Have in Common?
The murky yet promising future of the most programmable molecule in medicine.

On April 1, 2026, a Dutch expedition vessel called the MV Hondius left Ushuaia, Argentina, carrying around 175 passengers and crew into the South Atlantic. Ten days later, a passenger was dead. By the time the ship reached the waters off Cape Verde in early May, after a second passenger died onshore in Johannesburg and a third died on board, the World Health Organization (WHO) had declared an outbreak of Andes virus, a strain of hantavirus with roughly a 40% fatality rate and no approved treatment. Twenty-two countries coordinated an evacuation, while the Centers for Disease Control and Prevention (CDC) classified it a Level 3 emergency. Spain accepted the ship in Tenerife over the objections of the Canary Islands’ president, Fernando Clavijo. As of this week, passengers are quarantined in facilities from Nebraska to Zurich, and eleven confirmed or probable cases have been reported across multiple continents.

Moderna, the American biotech company that became a household name by producing one of the first mRNA COVID-19 vaccines, is once again in the spotlight.
On the day the outbreak made global news, Friday, May 8th, Moderna’s stock surged nearly 12%. By Monday, it was up another 7–9% in premarket trading. Then investors did the math — hantavirus doesn’t spread easily between humans, the WHO assessed public health risk as low, and analysts at Evercore ISI wrote bluntly that they saw “no meaningful revenue opportunity.” The stock gave back its gains by the close. A 20% weekly rally, then a retreat. The classic pattern: panic bids into a platform company, followed by the market remembering that a platform still needs products and demand…
But something real surfaced beneath the noise and stock trading rollercoaster. Moderna confirmed it had been working on an mRNA hantavirus vaccine, research that began well before anyone had heard of the Hondius. The stock, I think, spiked because of the belief that this company can quickly come up with solutions to new potential pandemics, and always has something in the drawer…
This belief is based on ribonucleic acid (RNA), or more specifically, messenger RNA or mRNA, the key information-delivery molecule in our body.
In this issue, we will explore why RNA is different from every other category of medicine ever built, how it was central to the most rapid fortune creation in pharmaceutical history, a world of new opportunities that can still unfold for it, the geopolitical power play in biotech, and the institutional wreckage that unfolded in recent years around mRNA technology.
Why is RNA so special?
In discussions about biology and life, we usually focus on DNA, deoxyribonucleic acid, a famous double-stranded structure that encodes all our genes.
Yet, an arguably much more promising molecule for many medical applications exists next to DNA — it is ribonucleic acid (RNA), a molecule that is very similar to DNA but has only one strand instead of a double-stranded structure, and a slightly different molecular alphabet.
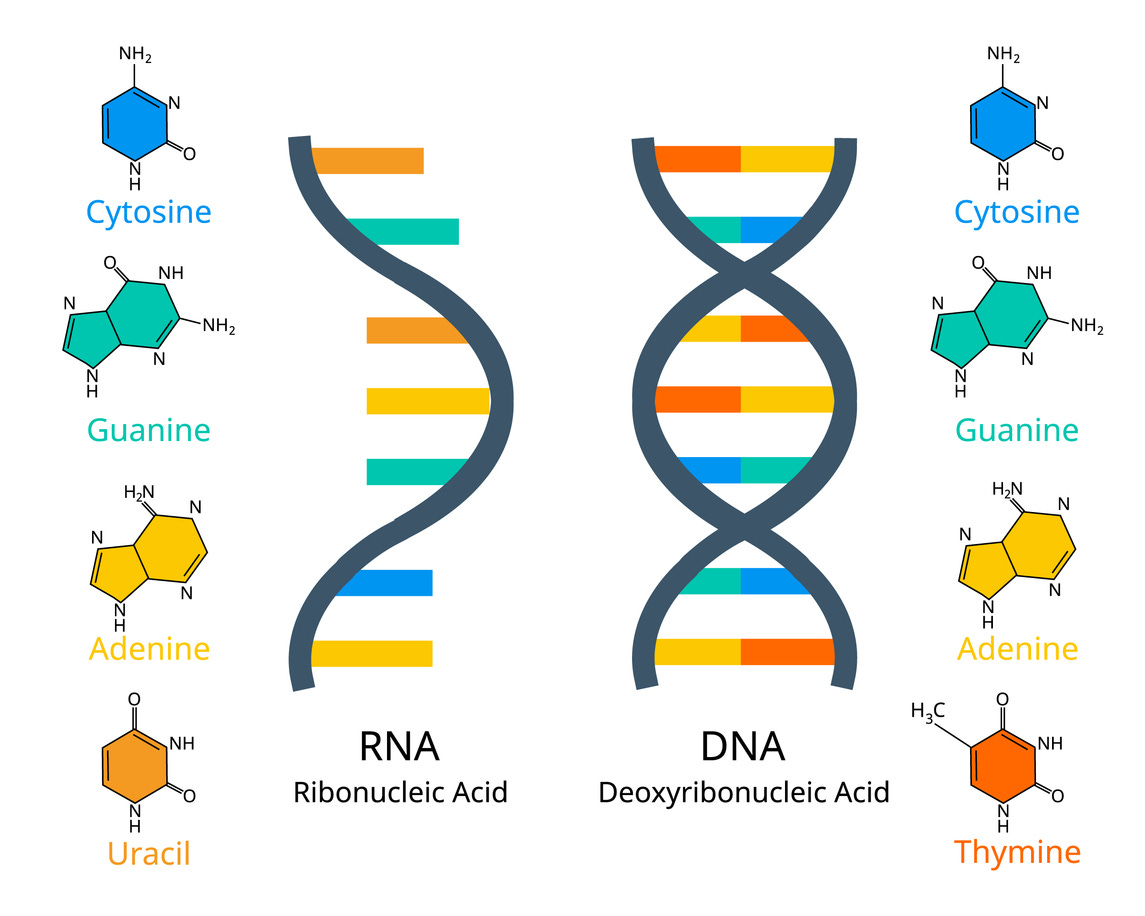
RNA comes in many forms — messenger RNA, transfer RNA, small interfering RNA, ribosomal RNA, and others. The one that concerns us here is messenger RNA, or mRNA: the temporary message that carries instructions from DNA to the protein-building machinery.
Zooming out a bit, our body runs on a straightforward molecular information chain. DNA is the permanent archive of information, the master copy of every instruction your cells will ever need. mRNA is the working copy, i.e. a temporary message that carries a specific instruction from the archive to the cellular machinery, a “printer for proteins” called the ribosome. Proteins are the result, the molecular components that do the actual work: building tissue, fighting infection, running metabolism, etc.
A bestselling science writer, Dr. Siddhartha Mukherjee, explains this beautifully in his book “The Gene: An Intimate History, “ which I'd highly recommend.
Now, for most of pharmaceutical history, drug companies have targeted proteins as the most straightforward way to influence biology, that’s what a typical medical pill does.
You swallow a pill that contains a small molecule, the substance travels through the bloodstream, and it interferes with a “misbehaving” protein. Say, Statins block a cholesterol-producing enzyme. Ibuprofen blocks an inflammation enzyme, etc. The approach works, but it is a “one size fits all” strategy. The molecule goes everywhere in the body, hits its target but also hits things you didn’t intend (which leads to toxicity or side effects), and wears off quickly, so you take another pill tomorrow.
Gene therapies aim at the other end of this spectrum: the DNA itself.
If you can rewrite the master archive, you can potentially fix the problem permanently, in the genes. Correct the initial blueprint, and it never triggers production of the wrong protein in the first place. Elegant in theory. In practice, it means making a permanent change to someone’s genetic code, which raises the stakes enormously. If something goes wrong, you can’t undo it. The regulatory bar is high, and the cost can be staggering. For instance, some gene therapies, like Zolgensma, are priced above $2 million per patient…
In contrast, RNA-based therapies and vaccines sit in the middle, having the best of both worlds.
In the case of mRNA vaccines, they are the message itself, written to do a specific job on the printer. The entire idea is to intervene at the messaging stage, between the blueprint (DNA) and the machine that builds proteins (ribosome), and introduce a new message to produce a protein the body wouldn’t make on its own.
And here’s the key property: the message shreds itself when the job is done.
mRNA degrades in the body within hours to days. It tells your cells what to build, they build it, and the instruction disappears. That impermanence is the entire strategic advantage!
Why? Because RNA gives you the precision of gene therapy, you can instruct the body to make essentially any protein, including ones it wouldn’t produce on its own, but with the reversibility of a conventional drug. If something goes wrong, you stop dosing, and the effect fades.
Crucially, because RNA is essentially a sequence of four chemical letters in different arrangements, designing a new one is closer to writing a line of code than to synthesizing a chemical compound. Change the sequence, change the instruction.
The four-billion-year-old platform
Now, using RNA to modulate biology, especially after the COVID pandemic, is often hailed as a revolutionary pharmaceutical idea, but it may be the oldest trick in biology, after all.
In May 2025, a team led by chemist Matthew Powner at University College London published a study in Nature showing that RNA can chemically link to amino acids (the building blocks of proteins) under mild conditions in water, without enzymes, without cells, without any biological machinery at all. The chemistry works at neutral pH, in environments like pools, lakes, or wet shorelines. It even works in ice!
What the researchers demonstrated is a plausible mechanism for how, roughly four billion years ago, RNA could have begun constructing the first crude proteins, essentially bootstrapping the very relationship between genetic information and functional molecules that every living cell on Earth depends on.
Whatever the final verdict on the origin of life turns out to be, RNA remains the most ancient messaging system in our biology, potentially older than DNA replication, older than the first cells. Worth keeping in mind when we talk about mRNA technology as something radically new…
Anyway, everything that follows — the fortunes, the patent wars, the geopolitical contests — flows from the RNA’s molecular logic.
The fastest fortune ever made… and lost
Before January 2020, Moderna was a company that most people outside the biotech industry had probably never heard of. Founded in 2010, it had spent a decade building an mRNA platform and burning through investor capital. It had never brought a single product to market. Its market capitalization at the end of 2019 hovered around $5–6 billion, respectable for a clinical-stage biotech, but surely modest by pharmaceutical industry standards.
Then the COVID-19 pandemic hit.
On January 11, 2020, Chinese scientists published the genetic sequence of SARS-CoV-2. Within 48 hours, Moderna’s team had designed an mRNA vaccine candidate. They did not need cell cultures or egg-based production or years of iterative chemistry… They took the viral sequence, identified the spike protein, wrote the corresponding mRNA instruction, and had a candidate ready for manufacturing. The first clinical batch was shipped to the National Institutes of Health for testing on February 24, 42 days (!) after the sequence was published. Those in drug discovery/biotech know that it is almost instantaneous, compared to a typical multiyear timeline.
That speed had a decade-long backstory, I’d like to revisit.
Katalin Karikó, a Hungarian-born biochemist, had been trying to make mRNA work as a therapeutic tool since the late 1980s. For most of that time, nobody cared. At the University of Pennsylvania in the 1990s, she applied for grant after grant and was rejected. In 1995, the university gave her a choice: stop working on mRNA or accept a demotion. She was being treated for cancer at the time, and she took the demotion.
What kept her going was a serious problem with the mRNAs: the body’s immune system treated synthetic mRNA as a foreign invader — it triggered inflammation and destroyed the molecule before it could deliver any instructions. Together with her collaborator Drew Weissman, an immunologist she met at a photocopier in Penn’s medical school, Karikó spent years testing chemical modifications to RNA’s building blocks. In 2005, they found one that worked: swapping uridine for pseudouridine let synthetic mRNA slip past the immune system undetected.
It was the foundational insight behind every mRNA vaccine that would follow.
Ironically, no major journal wanted the paper, and after it was published, almost no one cited it, and no wave of funding materialized. In 2013, Karikó left Penn, she said the university told her she was “not of faculty quality” — and joined a small German startup called BioNTech. In 2023, she and Weissman received the Nobel Prize in Physiology or Medicine. Every mRNA vaccine injected during the pandemic traces back to that chemical modification…
Anyway, what followed the rapid introduction of the mRNA vaccine during the COVID-19 pandemic was, perhaps, the most compressed wealth-creation event in pharmaceutical history. Moderna's revenue went from $803 million in 2020 to $18.5 billion in 2021 and $19.3 billion in 2022, almost entirely from a single product. Its market capitalization briefly approached $200 billion. A company that had never sold a drug before the pandemic was suddenly generating more revenue than some century-old pharmaceutical giants!
BioNTech, Moderna's German counterpart, followed a parallel trajectory. In partnership with Pfizer, it developed Comirnaty, the other mRNA COVID vaccine, and briefly became one of Europe's most valuable biotech companies.
And then the wave broke.
As vaccination rates declined and the pandemic shifted from emergency to endemic, the revenue collapsed. Moderna’s annual revenue fell from $19.3 billion in 2022 to around $6.8 billion in 2023, then to roughly $3 billion in 2024. Its market cap dropped from nearly $200 billion at peak to under $15 billion at its lowest. BioNTech followed a similar descent. Pfizer launched a $3.5 billion cost-cutting program, closed facilities, and laid off thousands.
During the boom, investors likely priced these companies as platforms, the idea being that the same technology that produced a COVID vaccine in weeks could produce vaccines and treatments for cancer, rare diseases, autoimmune conditions, and essentially anything else. The platform thesis was that it was not a one-product company, rather, a new paradigm for making medicine.
When the COVID revenue disappeared, however, the market perception changed, expecting product and demand beyond the initial vaccine success, which has not followed the way the market anticipated. That question remains open, and the answer will determine whether the mRNA boom was a one-time windfall or the beginning of something much larger.
A (potentially) bigger play
These days, Moderna and Merck are developing a personalized cancer vaccine called intismeran autogene (also known as mRNA-4157 or V940). The concept is striking in its ambition: a doctor takes a biopsy of a patient’s tumor, sequences it to identify the unique mutations driving a specific cancer, and Moderna designs a custom mRNA instruction set, encoding up to 34 of the patient’s tumor’s distinctive markers, which is then manufactured and injected to train their immune system to recognize and attack those exact cells.
In January 2026, the companies reported five-year follow-up data from the Phase 2b KEYNOTE-942 trial. The combination of the personalized vaccine with pembrolizumab (Keytruda, a leading immunotherapy drug) reduced the risk of melanoma recurrence or death by 49% compared to pembrolizumab alone. The benefit held steady from the three-year mark to the five-year mark, which is a signal that the immune memory triggered by the vaccine may be durable.
These are promising results, of course. But the power story is in the new paradigm of manufacturing and the economic system it implies.
Traditional pharmaceutical economics are built on mass production.
You develop one molecule, prove it works, manufacture millions (billions) of identical doses, and distribute them globally. Economies of scale are the foundation of the entire business model, and that’s how a pill can cost pennies to produce.
A personalized cancer vaccine inverts this logic entirely. Each dose is designed for one patient, so manufacturing is bespoke.
The production timeline is measured in weeks, not years, but the production run is measured in single doses, rather than millions. If the Phase 3 trials (now underway in melanoma, lung cancer, bladder cancer, and kidney cancer, with over a thousand patients enrolled) confirm the Phase 2 results, the question would not be limited to “does it work?” It effectively shifts to “who builds the manufacturing infrastructure for millions of custom products per year?”
How do you price a treatment that is, by definition, impossible to genericize? And can health systems designed for mass-market pills absorb something this fundamentally different?
Early estimates suggest personalized cancer vaccines could be priced around $200,000 per patient. Moderna and Merck have said that if the Phase 3 melanoma data are positive (readouts are expected as early as 2026), they could seek approval and launch as early as 2027. If that happens, it will create a new category of manufacturing that has no real precedent in the pharmaceutical industry.
The RNA molecule is only half the story of the mRNA revolution
Now here’s the part of the RNA story that will determine who actually controls this platform. The thing is, RNA molecules, on their own, are useless as therapeutics or vaccines.
They’re fragile, easily destroyed by enzymes in the bloodstream, and can’t cross cell membranes on their own. If you inject naked mRNA into someone’s arm, it degrades within minutes and accomplishes nothing.
The solution that made the entire mRNA vaccine era possible is the lipid nanoparticles, or LNPs. These are tiny bubbles made from carefully formulated mixtures of fat-like molecules that encapsulate the RNA, protect it from degradation, and ferry it into cells.
The groundwork was laid over four decades ago by Pieter Cullis, a physicist-turned-biochemist at the University of British Columbia, whose lab pioneered methods for packaging delicate molecules inside lipid carriers and delivering them into cells intact.
Without LNPs, there are no mRNA vaccines, no mRNA cancer therapies.
Arbutus Biopharma and its affiliate Genevant Sciences hold foundational LNP patents. For years, they pursued Moderna through courts worldwide, filing infringement lawsuits across five international jurisdictions, targeting 30 countries, with a separate US case heading toward a jury trial in Delaware. Then, in March 2026, six days before that trial was scheduled to begin, the parties announced a historic $2.25 billion global settlement. Moderna will pay $950 million upfront in July 2026, with an additional $1.3 billion contingent on an appellate ruling. If the full amount is paid, it will be the largest disclosed patent settlement in pharmaceutical history.
That number tells you everything about what the delivery system is worth. The public debate during the pandemic was about vaccine safety and mandates. The private fight, the one that just produced a $2.25 billion settlement, was about who owns the molecular packaging.
And it’s not over: the litigation against Pfizer/BioNTech’s Comirnaty is still active, with a favorable claim-construction ruling for Genevant/Arbutus issued in September 2025. Comirnaty represents roughly two-thirds of global COVID mRNA vaccine sales to date.
The mRNA sequence is easy to design. Without the delivery technology, it’s just information with no way to become medicine. The chokepoint of the entire mRNA platform is the delivery. That chokepoint has geographic consequences…
During COVID, mRNA manufacturing was concentrated almost entirely in the US and Western Europe. China and India, dominant in generic drugs and conventional vaccines, were largely shut out.
Both are now catching up, albeit slowly, likely with a long-term focus in view. China approved its first domestic mRNA vaccine in 2023, but with the end of zero-COVID, its factories sit idle, and demand has evaporated. India's Gennova Biopharmaceuticals developed an indigenous mRNA vaccine and is now working on a self-amplifying RNA platform for Nipah virus with CEPI funding, but it's still preclinical.
In Africa, BioNTech has invested roughly $150 million in a modular manufacturing facility in Kigali, Rwanda. Moderna announced a $500 million plant in Kenya, though the project has stalled. The WHO set up a technology transfer hub at Afrigen Biologics in Cape Town, which has developed its own mRNA vaccine candidate entirely on the continent. Real money, real facilities, but BioNTech's Kigali plant runs on BioNTech's proprietary technology and will manufacture BioNTech's products. A factory is not the same as an R&D platform…
The capacity to produce mRNA medicine is slowly spreading across the globe; however, the capacity to design it, control it, and decide what gets made remains concentrated in a handful of Western companies… for now.
The trust factor
The speed of mRNA vaccine development was arguably the most remarkable technical achievement in the history of pharmaceuticals. From a published viral sequence to a manufactured vaccine candidate in a matter of days. From trial to emergency use authorization in under a year. These timelines were previously thought to be unlikely.
For a significant portion of the public, that speed was precisely the reason not to trust it, however…
Ironically, mRNA’s greatest scientific strength — programmability and speed of candidate design — became its greatest political vulnerability.
Regulatory systems designed for decade-long drug development timelines were asked to validate something built in months. Public health communication infrastructure, designed for slow-moving campaigns about established interventions, was asked to explain molecular biology to billions of people simultaneously while a crisis was unfolding. The gap between what the technology could do and what institutions could credibly explain was enormous. The institutions failed to manage the mRNA technology perception crisis because they were designed for a slower world.
The result is a trust deficit that now functions as a perception tax on the entire RNA platform. The tax is even quantifiable. A study of over 35,000 adults across nine countries found that the novelty of mRNA technology alone reduced the odds of vaccine acceptance by 14.2% compared to conventional vaccines — same disease, same efficacy data, different platform, measurably lower trust.
A 2023 global survey found that nearly half of respondents trust traditional protein-based vaccines more than mRNA vaccines. And the spillover extends beyond mRNA: MMR vaccination coverage among US kindergartners dropped from 95.2% to 92.7% between 2019 and 2024, leaving over 280,000 additional children unvaccinated and contributing to the highest US measles count since the disease was declared eliminated in 2000.
A KFF survey found parental skepticism toward vaccines had risen from 22% to 27% in a single year, with perceived politicization as the primary concern.
In 2021, Moderna hired its first-ever chief brand officer from Ogilvy Health, launched the global "Welcome to the mRNAge" campaign in April 2023, explicitly to counter vaccine hesitancy by explaining the science behind the platform.
Moderna's chief brand officer Kate Cronin told Marketing Week in 2023: "We lost relevance" — a remarkable admission from a company that had been, three years earlier, one of the most recognized names on Earth. In 2024, CEO Stéphane Bancel personally took over marketing during a leadership transition.
Zooming out of Moderna’s post-pandemic roller coaster, it seems like every future RNA therapeutic, including personalized cancer vaccines, cholesterol drugs, rare disease treatments, etc, might be introduced into a public discourse shaped by the COVID-era polarization. This is not merely a communications problem that can be solved with better messaging, but more like a structural cost baked into the economics and politics of mRNA products for the foreseeable future.
What comes next
The bigger picture emerging from this story is that mRNA is not just the COVID vaccine. It is a broad programmable platform for writing temporary instructions to the human body, potentially for various therapeutic applications, but also a quick instrument to prepare for future pandemics, and the race over who controls it, who profits from it, and who gets access to it is just beginning.
Here’s what to watch.
Cancer treatment may become personalized manufacturing. If the Moderna/Merck trials deliver, a patient’s tumor gets sequenced, and a bespoke vaccine is synthesized in weeks. That would go way beyond an incremental improvement on existing oncology; it would be a different category of medicine — one patient, one product — and no health system on Earth is currently built to pay for it or deliver it at scale.
Pandemic response may shift from years to days. The mRNA platform can generate a vaccine candidate within days/weeks of receiving a pathogen’s genetic sequence. We saw this with COVID. The constraint is not so much the technology, but more so the operational and manufacturing readiness, as well as public perception management.
Diseases that were never economically viable to target suddenly become feasible. Designing a new mRNA sequence costs almost nothing — it’s computational. The expensive part is manufacturing and clinical trials. That means rare genetic conditions, tropical diseases, pathogens that primarily affect poor countries — categories that traditional pharma has largely ignored because the market was too small — could become viable if the funding and manufacturing bottlenecks are solved.
The question of who controls the platform will shape who has access. The $2.25 billion LNP settlement, the idle Chinese factories, BioNTech’s Kigali facility running on proprietary technology, the stalled Moderna plant in Kenya — these are early moves in a long contest over whether mRNA medicine becomes broadly accessible or remains concentrated in the hands of a few Western companies and the nations they operate in.
None of this is guaranteed. The platform could stall on failed clinical trials, regulatory gridlock, or a trust deficit that proves deeper than anyone expected. The cancer vaccine data could disappoint. The geopolitical competition could fragment the platform rather than expand it.
But the underlying RNA tech capability is real, it is proven, and it is not going away. A molecular class that may have started life on Earth four billion years ago is now being reprogrammed in laboratories to address some of the hardest problems in medicine. Science is moving at the speed of information while everything else — the money, the politics, the institutions, the trust — is still catching up.
P.S. I read your piece a few days ago, and I haven't been able to stop thinking about it since.
At its biophysical core, an uncomfortable question remains: What happens when humans spend decades in environments optimized for economic throughput while losing the regulatory bandwidth their biology evolved to maintain?
When these systems eventually fail, we often engineer, patent, and sell back functions that evolution once provided for free. That is undoubtedly a medical achievement—but it also raises the question of whether we are treating the causes of dysregulation or merely commercializing its consequences.
Great article! Your metaphor of RNA as a programmable interface is a brilliant piece of systemic critique.
It’s a fascinating paradox: nature perfected this RNA mechanism over billions of years through self-organization. Our cells are naturally built to do this. But looking at how hard it is for so many people today to fight off viral infections, it shows one major thing: our modern, chronically stressed metabolic environment has systematically stripped our bodies of the baseline conditions needed for this ancient system to run smoothly.
Modern biotech has to step in with artificially programmed mRNA from the outside simply because we’ve robbed our internal biology of the bandwidth to manage the code from within.
Thank you!